- It is not OK to show your private parts to other people.
- It is not OK to look at other people’s private parts.
- It is not OK to touch other people’s private parts.
- It is OK to touch your private parts as long as it is in private and does not take too much time.
- It is not OK to use sexual language or make other people uncomfortable with your sexual behavior.
Learning the Private Parts Rules was very helpful. The rules helped him understand what is acceptable and what is not. Also he knows who to go to if someone tries to break the rules with him. -Parent of a 6-year-old boy
Caregivers are often uncomfortable about teaching accurate labels for private parts. There are a variety of labels , in addition to “pee-pee” and “poo-poo,” such as “cookie jar,” “chicken,” or “peanuts.” We recommend that all children learn the correct names for body parts, including private parts. Some of the reasons to teach the specific names, such as penis, testicles, vulva, clitoris, vagina, breasts, and buttocks, are as follows:
- It can be easier for children to report when someone has tried to touch their private parts if they know the correct words.
- It gives the message that these are just parts of a child’s body, rather than something that is problematic.
- It gives the message that body parts can be talked about directly with the caregivers, rather than being something hidden or vague (such as “down there”).
- Other names for private parts can be confusing for the children.
- Children can give more specific descriptions when they tell an adult about a physical problem (such as pain, itching, or other physical problems).
Caregivers may wish to use labels of body parts from languages other than English. For example, members of some American Indian tribes may prefer to use their tribal language when teaching about body parts.
It is important for a child to be able to describe what happened when he or she has been sexually abused. When children do not have accurate words for body parts, they are often unable to provide important details needed to protect them from abuse. Too often, young children can only report vague information, such as, “He hurt me down there,” and Child Protective Services and law enforcement are unable to accurately determine what happened. Help your children to become knowledgeable by teaching them accurate information about their bodies in age-appropriate terms. Help them to learn which adults they can talk to when they have questions or concerns about private matters.
One day while waiting in the checkout line at the grocery store, my 4-year-old son bumped into the basket and then started singing, ‘I hit my penis! I hit my penis!’ At first, I was mortified. But then I realized, it’s just part of his body, and I’m glad he knows the name, in case anything should ever happen to him. I looked at the checkout clerk and other customers, and they smiled knowingly—young active boys are just that way. Afterwards, I talked with my son about public and private language. -Parent of a 4-year-old boy
There can be downsides to teaching young and especially impulsive children the correct terms for private parts, because sometimes these children will use the terms in public. Teaching children public and private language as well as public and private behavior can help. The reasons for teaching the correct names, however, outweigh a little public embarrassment if your child talks about or asks about private parts in public.
Young children will benefit from information that they can see or touch. We have found it helpful for children to understand the general term “private parts” and to learn that these are the parts of our body that we keep covered when around other people, even when we are swimming. Our bathing suits cover our private parts.
It has helped Maria to learn more about her private parts, and why she should not show them or see others. -Parent of a 6-year-old girl
Learning the Sexual Behavior Rules helped him to realize rules of proper behavior in a manner any child can understand. -Parent of a 10-year-old boy
Pictures of children in bathing suits such as this one can help your child to visualize where his or her private parts are.
Here are some of the things you can do to help prevent future problematic sexual behavior, by using Private Parts Rules or Sexual Behavior Rules:
- Develop specific rules for your family, worded in a manner that you are comfortable with. Name the rules something that you can refer to in public, to help remind your children to follow the rules, such as the Bathing Suit Rules, or Privacy Rules.
- Rehearse the rules at home to help your child understand that these rules apply to home life as well as to group situations. Many rules in your children’s lives will differ, depending on where they are (for example, rules at the park are different from rules at Grandma’s house, which are different from rules at home). Your children need to learn that Private Parts Rules are always in place, no matter where they are.
- Have a regular “family time” at home in which your family checks in about how things are going in general and ends with a fun activity. At these family times, periodically check to see if your children are able to recall the Private Parts Rules.
- Praise your children for their positive behavior. When they are being good, let them know what they are doing well. For example, if your daughter has been getting into the physical space of her siblings (such as constantly wanting to hug and kiss them), praise her when she plays well with her siblings and leaves respectful spaces between their bodies.
- Have an agreed-upon gesture or word that you can use when your children look like they are about to violate a Private Parts Rule. This approach is most useful for behaviors that are frequent. A caregiver may use a hand signal (such as pointing up) or a verbal cue (such as saying, “Remember the Bathing Suit Rule”). The cue should be decided with children before a caregiver uses it so that the children know what the cue means.
- If your children come to talk with you before breaking a Private Parts Rule, praise them. Encourage them to talk with you any time they are struggling with the rules. Decide together what each child will do to obey the Private Parts Rules.
- Encourage activities that make breaking Private Parts Rules unlikely for your children during times when they are most likely to act out. These activities can be:
- ones that use energy, such as bike riding, running,
- or playing catch (avoid body-contact activities, such as wrestling, tickling, or roughhousing)
- ones that take concentration and that will distract your child (non-violent video games are sometimes good, as well as the game “Concentration,” or board games) and
- ones that provides appropriate physical nurturing, like holding hands, stroking your child’s hair, or patting your child’s back (this kind of caring touch can help fill a need for physical contact in appropriate ways).
- Use redirection, reminders, and distraction. For example, if your child looks like he might make a poor decision, redirect him to something he should be doing instead.
- Let your child know what the consequences will be for breaking the Private Parts Rules. Not every behavior needs a time-out. Make the consequences relate logically to your child’s behavior, if possible. For example, if you catch your child watching an “R” rated movie on television, the consequence could be that he cannot watch television for the next couple of days.
- Ask for support from others in your child’s life (daycare workers, babysitters, friends, teachers, and relatives) to reinforce the Private Parts Rules.
My 7-year-old son was playing with his same-age cousin. I heard him say, ‘Let’s play boyfriend and girlfriend.’ I knew that this could lead to a big problem. I grabbed some puppets, put them on my hands, jumped behind a chair, and started acting out a puppet show. They got so excited they wanted to make up their own puppet shows, and they played with the puppets for the next hour! Distraction really worked! -Parent of a 7-year-old boy
Respecting Other People’s Space: Teaching Good Boundaries
Children with problematic sexual behaviors often have trouble knowing when they have moved too closely into another person’s space or physical boundary. Getting into other people’s personal space causes them problems with other kids and with others at school and at home. For example, these children may have trouble keeping their hands to themselves, and may frequently touch the people around them. Or they may be the kind of children who run up and give a big hug and kiss to a stranger they just met, such as Summer in the third example. Not only is this behavior disrespectful of the other person, but it is also risky, because such children may be more vulnerable to being targeted by adults with intentions to harm them.
Thus, it is important for children to learn to respect other people’s physical boundaries and to protect their own. Such knowledge is especially important for children with a history of problematic sexual behaviors. The idea of “boundaries” is fairly difficult for young children to grasp. One method that makes it possible for a young child to visualize his or her “space” is to use a hula hoop. (If you use a hula hoop to teach boundaries, though, first allow your child to play with it, or the child will have difficulty paying attention.) If you do not have a hula hoop, demonstrate “space” by holding out your arms level with the ground.
- Have your child sit in the middle of the hula hoop.
- Explain that all people have “space” around them, and that they have the right to say who can be in the space and who can’t.
- Explain that when someone else enters that space without permission, the person inside the space often feels uncomfortable.
- Give your children words to use to ask before going into someone else’s hula space, such as, “May I give you a hug?” or “May I sit here?”
- Give children assertive (not too aggressive or too passive) words to use to tell other people to step out of their hula space, such as, “Please move over.”
- Teach children ways to greet people that do not involve hugging or sitting in their laps. They can hold out their hand and shake hands. Such greetings can be made more personal for special people, by using something like a high five.
Individuals in families, churches, and other cultural and community groups have their own greeting rituals and areas of comfort regarding physical space. Some groups remain at arm’s length when their members get together, while people in other groups stand right next to each other when talking, even though the people might have just met. Some church communities greet members with a hug and kiss on the cheek. There is no “right” response to managing these different community rules for all children with problematic sexual behaviors. With professional support, you can develop rules and teaching strategies that fit your own children. Older children often can learn different greeting rituals for different groups of people, whereas younger children or impulsive children may not understand why they can hug some people they know but not others.
Children need to know how to respond when they feel someone has gotten too close to them. Further, they should be taught to respect others’ wishes for greater physical space.
Guidelines To Follow If You Find Your Child Engaged In Sexual Behavior
By using the guidelines and rules above, and by keeping close visual supervision of your child, most problematic sexual behaviors can be prevented. If supervision becomes lax or if for some other reasons your child displays an inappropriate sexual behavior, the following list provides some guidelines for responses.
- Try to remain calm and keep an even volume and tone of voice. Count to ten, take deep breaths, or use other strategies to help calm down. When you remain calm, it helps you to have better responses than when you react with strong emotions. When you remain calm, it helps your child to understand that it’s the behavior you don’t approve of, not the child.
- If needed, have the children get dressed and go to separate areas of the home.
- After you have all the children dressed and in a safe place, check your level of emotions again. If you are in control and at least somewhat calm, proceed with the steps listed below. If you continue to be very upset, find some outside source of support, such as a professional, a partner, or a friend. Continue to take deep breaths.
- Once calm, evaluate the situation. Ask the children individually what happened. Keep the questions open ended so that they can tell you in their own words (rather than just by answering yes or no). Ask things like: What happened? Who thought of doing this? How did you learn about this?
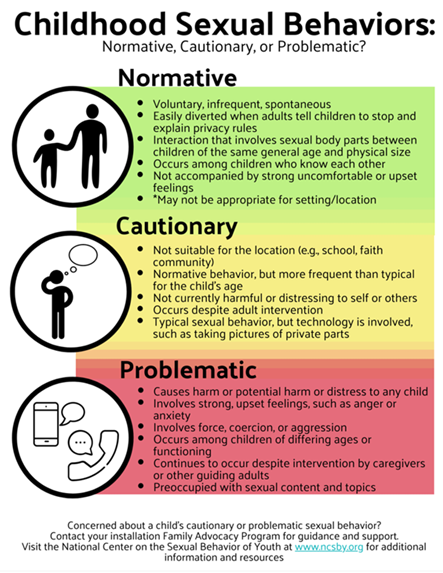
- Try to determine how problematic the behaviors were (when is sexual behavior a problem?).
- If your child, who initiated the behavior, has been taught privacy rules, remind your child of the specific Private Parts Rule that he or she is breaking (for example, “Remember, no touching others’ private parts”).
- If a consequence is necessary, provide it immediately in a firm, but calm manner, such as, “Because you tried to touch Tommy’s private parts, Tommy has to go home, and you can’t play with him for the rest of the week.”
- After the consequence, help your child to think of things that he or she could have done instead of the sexual behavior, such as talking to an adult, playing with a toy, or drawing a picture.
- Let your child know that you believe in his ability for self-control. Emphasize that he can try something different next time. “Next time you think about touching Susie’s private parts, you can play ____________ instead, or you can come ask me for help.” Give your child the words to say and practice them with him.
- Determine if consequences are not necessary and redirect your child to another activity. If the behavior is okay when done in private (such as when a child touches herself), redirect her to her bedroom or to another nonpublic place.
- Talk with the caregivers of the other children involved, if appropriate.
- Praise your child during times when he or she displays positive behaviors.
- Remember that children with problematic sexual behaviors always need close visual supervision when with other children.
Developing A Support Team: Communicating With Other Adults
Raising a child who has had problematic sexual behaviors can bring great stress paired with a sense of isolation to the caregivers. Children’s sexual behavior is a hard topic to talk about with other adults. It is important for you to have at least one other adult that you can talk to in private about your child’s sexual behavior and about your thoughts, feelings, fears, beliefs, and other related topics. Children are cared for by multiple adults (including teachers, parents of the children’s friends, neighbors, and relatives). These adults will need to know the appropriate level of supervision to provide. But no single rule can be applied to all children who have had a problematic sexual behavior. Decisions about who should be included in the support team will differ depending on the child and family situation and context.
A wider net of support is needed for children who
- Have had frequent or impulsive problematic sexual behavior in a variety of settings (such as at home, at school, and at daycare), because they will need closer visual supervision
- Have poor decision-making skills and combative behavior
- Have demonstrated aggressive or demanding behavior or
- Have significant developmental issues.
While it is important for you to have other supportive adults with whom to discuss the details of these situations, it is not necessary for all adults in your child’s life to know details about the behavior. In fact, in some cases, it may be harmful for certain adults to know the details of your child’s past trauma experiences and sexual behaviors, especially if those adults use the information to label and make fun of the child. Typically, the information that needs to be shared with other adults is that
- Your child has a history of making poor decisions when unsupervised with other children. At times it also can be helpful to tell those other adults that things have happened in the past to the child, which have interfered with his/her ability to make good decisions with other children (such as abuse)
- Visual supervision is needed to make sure all children are safe
- A plan is needed to prevent potentially risky situations, such as having an adult always accompany your child to the bathroom and insure that he or she is not alone with other children and
- Other safeguards may be needed in situations that typically have lower levels of supervision (such as playing on the playground).
Potentially Risky Situations
Over the years, we have found some situations more risky for a child who might be inclined to engage in a problematic sexual behavior again. By being aware of these potentially risky situations, you can better plan to avoid them or to incorporate safeguards and supervision to prevent future problematic sexual behavior. High-risk situations include the following:
- Sleepovers
- Contact sports, such as wrestling
- Holiday times
- Summer vacations (which are less structured than school environments)
- Camping
- Recess, when poorly supervised
- Summer camps
- Shared bathrooms at school, etc.
- Cell-phone use
- Unstructured, poorly supervised activities
- Poorly supervised Internet, video game, or television time
The level of supervision and information provided to the supervising adults will differ depending on the needs of your child. Typically, until your child with problematic sexual behaviors has a long period of demonstrating good boundaries and decision making, and maintaining rules about sexual behavior (over a period of time of at least three months), the risky situations noted above should be avoided. If situations cannot be avoided while the children are continuing to demonstrate problematic sexual behavior, maintain visual supervision when your child is with other children.



 Treatment works!
Treatment works!




